Cerebellar Development, Function and Injury
 Premature infants born earlier than 32 weeks with very low birth weight or VLBW (<1500 g) are highly vulnerable to developmental delay in sensory, cognitive and motor processing. Perinatal insults such as hypoxia (low O2) affect the developmental program of specific neuronal populations resulting in behavioral deficits. Between 24 to 32 gestational weeks, the cerebellar cortical surface area expands rapidly. Cerebellar circuitry, therefore, is prone to injury-related dysfunction during this time window. Clinical data indicates that VLBW infants are 40 to 100 times more likely to develop locomotor deficits than term infants. Using an established chronic perinatal hypoxia (Hx; 10.5% O2 from P3-P11) mouse model of neonatal brain injury, we previously identified a GABA-dependent developmental disruption of the cerebellar white matter. We also discovered a delay in the development of Purkinje cells (PCs), which constitute the sole output of the cerebellar cortex. In order to characterize potential behavioral and physiological consequences of PC developmental disruption, we are now using our model to investigate locomotor deficits and changes in PC electrophysiology, and how PC abnormalities are causally associated with locomotor impairment. We hypothesize that perinatal brain injury (Hx) leads to adaptive cerebellar behavioral deficits caused by abnormal Purkinje cell development and physiology.
Premature infants born earlier than 32 weeks with very low birth weight or VLBW (<1500 g) are highly vulnerable to developmental delay in sensory, cognitive and motor processing. Perinatal insults such as hypoxia (low O2) affect the developmental program of specific neuronal populations resulting in behavioral deficits. Between 24 to 32 gestational weeks, the cerebellar cortical surface area expands rapidly. Cerebellar circuitry, therefore, is prone to injury-related dysfunction during this time window. Clinical data indicates that VLBW infants are 40 to 100 times more likely to develop locomotor deficits than term infants. Using an established chronic perinatal hypoxia (Hx; 10.5% O2 from P3-P11) mouse model of neonatal brain injury, we previously identified a GABA-dependent developmental disruption of the cerebellar white matter. We also discovered a delay in the development of Purkinje cells (PCs), which constitute the sole output of the cerebellar cortex. In order to characterize potential behavioral and physiological consequences of PC developmental disruption, we are now using our model to investigate locomotor deficits and changes in PC electrophysiology, and how PC abnormalities are causally associated with locomotor impairment. We hypothesize that perinatal brain injury (Hx) leads to adaptive cerebellar behavioral deficits caused by abnormal Purkinje cell development and physiology.
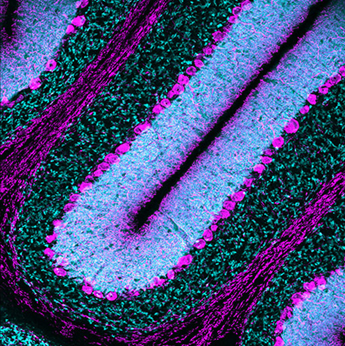
Postnatal cerebellum. This image shows Purkinje cells in magenta labeled with an antibody against Calbindin. Cyan denotes vesicular glutamate transporter 1 (VGLUT1) which is expressed in mossy fiber rosettes and parallel fibers, which make en passant synapses on Purkinje cell dendrites.